This is the presentation that Marilyn Chow, Marilyn Chow, DNSc, RN, fAAN, Vice President of Patient Care Services, and I gave at the DC Health Innovation Summit, part of 2011’s DC Health Innovation Week.
I am not the hugest fan of Slideshare’s formatting, so I’m including as a series of images below, as well as with a transcript on the bottom. Enjoy, feel free to embed.











Marilyn: Hi, I’m Marilyn, Vice President, Patient Care Services, for Kaiser Permanente
Ted: Hi, I’m Ted, a Director in The Permanente Federation of KP Medical Groups
M: Welcome to the Kaiser Permanente Center for Total Health. Many of you wondered if you would get time to experience the Center during your time today.
T: With that in mind, we would like to spend the next 30 minutes introducing you to five innovations that are portrayed on the Center’s digital walls, and to people here from Kaiser Permanente who you’ll want to meet and learn more from.
M: The Kaiser Permanente Innovation System is people, spaces, tools, networks, methodologies that an organization has in place to support continuous innovation. It’s in our DNA, which means that any problem we encounter, whether identified by our senior leaders or our frontline staff, is seen as an opportunity to make patient care better, more affordable, more accessible.
With that in mind, let’s start the list.
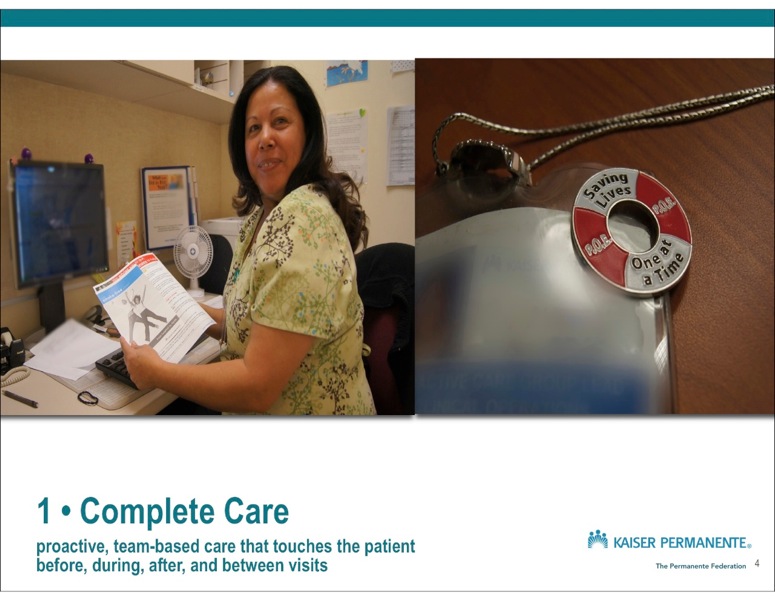
The first innovation is Complete Care. Complete Care includes Proactive Care, which touches the patient, before, during, after, and in between visits.
Kristen Andrews is here, from Southern California Permanente Medical Group where she is the Regional Proactive Care Group Lead.
Includes: Proactive Panel Management, Proactive Office Encounter (Outpatient visits), Proactive Inpatient Encounter (Inpatient visits), Proactive Office Support, as well as condition management leads for Diabetes, Asthma, Hypertension, HIV, and chronic kidney disease.
You shouldn’t have to have luck in order to have your life saved in our health care system. 2/3 of the time a patient presents with a gap in care, it’s to specialty.
Michael Kanter, MD told me that when he brought up the idea of specialists doing primary care, they looked at him like he was from Mars.
In 2008, Kaiser Permanente Southern California was #1 in the United States in breast cancer screening % for women. In 2009, they were surpassed by….Kaiser Permanente Hawaii. In 2010, KP Hawaii was surpassed by…Kaiser Permanente Georgia, all well above the 90th percentile of health plans, with KP Georgia being #1 in the United States.
On the left is a photograph of Elsa Torres, a medical assistant at Barranca Medical Center, Irvine California, when I asked her what this means, she said “Some people work to cure people, we work to keep them from getting sick”.
On the right is a photograph of Kristen’s badge, the same pin I am wearing on my jacket. It says “POE, Saving Lives, One at a Time.” I first visited KP Southern California to learn about Complete Care a year ago in San Diego at Rancho Bernardo, and I kept hearing people say “this is about saving lives.” The same was the case on a visit to Orange County this year.
Even the language they use is truly patient centric – they speak about prevention, teams, and tools in ways that humans can understand.
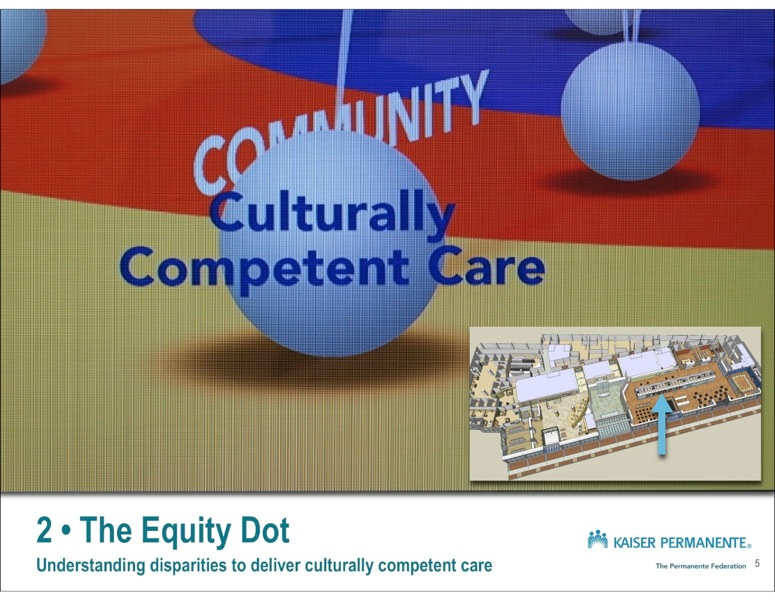
The Second Innovation is….Equity Dot
Raymond J. Baxter, PhD, is Kaiser Permanente’s senior vice president for Community Benefit, Research and Health Policy. . Dr. Baxter leads the organization’s activities to fulfill its social mission, including care and coverage for low income people, community health initiatives, environmental stewardship and support for community-based organizations, as well as research and the Kaiser Permanente Institute for Health Policy.
The equity dot is literally a “dot” on the Kaiser Permanente Quality dashboard, called “The Big Q.” The equity “dot” adds the measurement of disparities to the measurement of performance, across 16 HEDIS measures.
Ray Baxter has led KP’s work on health equity and elimination of health disparities. It’s because of him that our key quality measures can be broken out by race, ethnicity, gender, compared to benchmarks, and trended over time. This fits into the six aims of Quality in the Big Q: safe, effective, efficient, timely, patient-centered, AND equitable care. Continuing on the theme of breast cancer screening, we have documented that ALL racial/ethnic groups are above the 90th percentile of health plan members in receiving recommended mammography, and a gap between white women and African American women no longer exists.
From this measurement work, innovations towards identifying practices and tools to address health care disparities have coalesced through the ECHO work (Equitable Care Health Outcomes), that Ray can tell you about.
What do you do when you have a commitment to Total Community Health and you’re confronted with the shocking statistics around racial and ethnic disparities in health care?
On the left is a call to action from Kaiser Permanente about the overdue attention to disparities in health care. On the right is a map generated by Kaiser Permanente Care Data Analysis showing the link, among KP members between place, poverty, and obesity in the East Bay.
We know that Total Health requires equity and social and economic well-being, which includes the care we provide, as well as supporting the environment beyond the the doctor’s office.
Scott Young, MD, is the Associate executive director, Clinical Care and Innovation, The Permanente Federation, LLC
This is an example of the patient centered transitions bundle. Dan Hyunh, MD, leads a follow-up call program staffed by MD’s, nurses, and pharmacists, making sure that medications are understood, appointments are made, and if needed, changing and documenting in the electronic health record bridge between hospital and next encounter. Dan told us that his team will provide feedback to hospital teams and they will change their process as a result. For example, looking at the IV antibiotics example, were sharps disposal containers provided with discharge? This was something we learned when care teams saw the impact from the patient perspective.
We started this dialogue talking about people, spaces, tools, networks, methodologies.
Now I would like to tell you about some of our people and our processes.
Starting in 2003, we worked with IDEO and developed Innovation Consultancy to bring human centered design in house. Human centered design is when you tackle problems by first observing the needs of your users.
I would like to mention two specific processes developed through the Innovation Consultancy work.
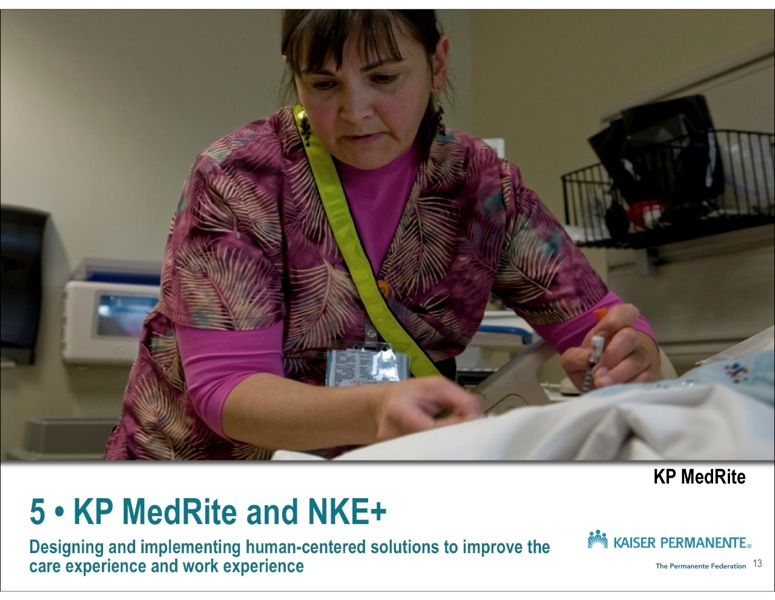
The first is KP Medrite. Imagine that you have installed a state of the art electronic health record with barcode medication administration, as many hospitals are today. Are the problems with medication administration in the hospital solved?
We learned from our research that 17% of a nurse’s time is spent doing medication administration, and it was unclear, chaotic and full of interrupts. Through observation, prototyping, and co-design with our nurses, we developed a simple, elegant, and safe solution, which we call KP MedRite.
In the photograph above, you can see one of our nurses with “no interruption wear” on her body. It is a signal that the nurse is engaged in administering medications, she or he is not to be interrupted.
The sash is the sexy part of KP MedRite; there are three other components that Chris or Christi can tell you about.
The second Innovation from the Consultancy I would like to tell you about is Nurse Knowledge Exchange Plus.
Using the same techniques used to develop KP Medrite, we worked to solve the problem of not enough time at the bedside for nurses. We brought nurses out of the conference room and to the bedside in 2004 with Nurse Knowledge Exchange. The “plus” came in 2009 when the Consultancy worked with nurses and the entire unit to protect and optimize patient-nurse interaction during shift change.
The results are a 20 % increase of nurse time spent in patient rooms, 19 % decrease of nurse time spent at the nurses’ station. Patients and families feel involved in their care, and nurses are able to focus on the priority of getting a good safe report and being with patients.
Both of these projects have placed freely downloadable, comprehensive change packages on our external web site.
M: Ted, there’s one more innovation
T: Yes, Marilyn. That’s the original innovation that created Kaiser Permanente – Prepaid, integrated, comprehensive health care. You can learn about it in the orientation center.
This is Sidney Garfield, MD, around 1938, and a little part of his story:
“Unable to make ends meet on the usual fee for service, I finally tried prepayment and thus happened on our basic concepts of health care. The people, with the barrier of cost removed, were coming to us earlier. We were able to treat them earlier, prevent them from getting complications and keep them from dying.” (1945)
On The right is a prototype of a new type of medical office – this prototype was built inside the Garfield Center for Health Care Innovation. 11 of them are now operating in Georgia.
On the lower right is a sign showing how our heritage is reflected in everything we do. At the State of the art Kaiser Permanente Irvine Medical Center, the roads are named “Prevention Way,” and “Wellness Way.” These are actually labeled as such on Mapquest. I took a photograph of this because I remembered that at another hospital I once visited, the side road was called “Top Doctors Way”.
5 Comments
leaders. “@tedeytan: The Kaiser Permanente Innovation Journey – from #futurehealth – DC Health Innovation Summit http://t.co/aLlJVxH”
RT @tedeytan: Preso: The Kaiser Permanente Innovation Journey: from #futurehealth – #DCHealth Innovation Summit http://teyt.in/lQOZ2f
Hi Ted,
I wish I could have been there in person and get to visit that new awesome space.
I was impressed with the "equity dot" feature because I have been puzzling over how to make use of disparity data and present such information in a way that is meaningful and actionable by doctors. I realize how it totally makes sense that this innovation is emerging in the super diversity mix of the East Bay Kaiser Permanente. I would love to hear and learn more as this evolves.
Just read an article about how being a new single mother can lead to poor health outcomes and my buddies have taught me a lot about LGBTQ health disparities as well. I wonder what would make sense in how to share one's personal profile so that a doctor could be aware of all the social/population factors that go into health disparities?
Yin
Hi Yin,
Great question – I think given your expertise you would have really been interested in one of the breakouts at the Health Innovation Summit, convened by Lyle ("Dr. Lyle") Berkowitz (@drlyle1) – he wanted to talk about EHR apps and a health app store that could be used for the purpose of expanding the functionality of EHRs in specific ways. One of the things we mentioned was an app that could bring in GIS or other relevant data from the patient's life and add it to the display so a physician could be aware of specific vulnerabilities. I suppose the same could be done if a patient decided to host a profile somewhere (or on their mobile phone) that had a secure link to the EHR system of the future. I guess kind of like BUMP, a patient could release targeted sections of their profile to their physician, and hopefully with greater trust, as much as is useful for them to get culturally competent care.
I still think the mobile phone offers more opportunity for the patient to bring the personal into the personal relationship. What do you think in your zip-health-ness?
Ted
In my work with community people working on environmental health and justice – we often talked about how where we live, work and play affects our well-being and health. Living next to oil refineries, freeways could be the cause of asthma – and no matter the medication compliance, the source of suffering is unjust pollution. I think there could be some interesting mash ups between the EPA's data, HHS Health disparities data, and having patients share short narratives as part of their PHR record about their living situation. Perhaps even sharing images and GPS mapping of one's living environment as part of a medical record. I've been playing around with how to capture the the idea of medical narratives in the PHR and how telling one's story is part of feeling heard and cared for by the medical system.
Thanks for the connection. I will get in touch with Dr. Berkowitz as soon as I catch my breath – always look forward to meeting curious and inventive souls.