
Imagine how strange it is to read this article after seeing this issue come alive through the storytelling of @ReginaHolliday at Health 2.0 STAT DC last week. It’s hard for this (or any) written description to fully capture the agony and devastation caused to families through opacity in health care:
Many clinical institutions charge for copies, authorize patient review only when a clinician is present, and take their time responding to patient requests for records.
For comparison of impact, look at the 73 Cents Mural and decide for yourself.
However, there’s a lot going on here, including a compelling story. This story includes people, and the researchers on this project are top notch, thoughtful, interested in applying their talents for the benefit of patients everywhere (some of them even trained me … ).
The story also includes an intervention, which is the actual opening up of patient medical records, or actually a part of it, the part that has traditionally been the most secretively kept by health care professionals. The article describes the challenges of sharing doctors’ notes with patients and even has a diagram showing all the people who have access to the notes today. It appears that a lot of people do, just not the patient. Take a look.
In thinking of the experiences right next to each other (Regina and this paper), I quickly diagrammed all of the things that may impact the eventual opening of the doctors’ note to patients and families online for me to visualize the situation better (click to enlarge):
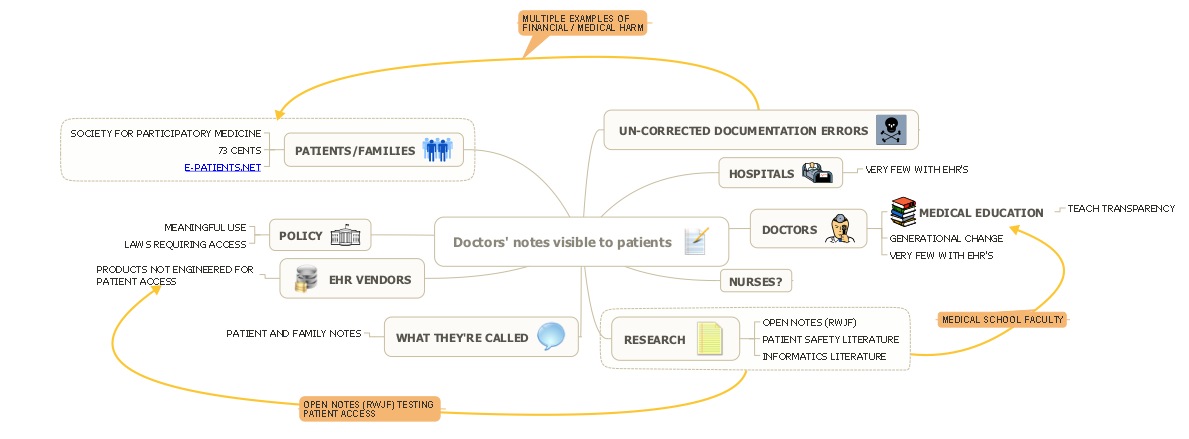
First realization: “Yet another diagram with the patient not in the center,” and “we’re hyperfocused on one aspect of a medical tool (whether patients can see it), not on how we use it to help patients heal.”
Second realization: There’s a lot of “stuff” in there. Does it seem a little bit like we’re actors in a play based on a script we didn’t write? Where did the norm of secrecy come from and why have we made ending it so complicated – I have recounted that I “learned” that patients were not supposed to see their notes in high school, not in medical school. (To the nurses and doctors reading this, when did you actually “learn” that patients were not supposed to see their medical records? Did someone teach you, did you read it somewhere, or did you learn from an experience? – post in the comments, please. )
A research study is a good way to change norms, and this group, through the incentive of grant funding, is changing the wiring of several electronic health record systems to try out a new way. That’s significant in the path to changing norms. The other significant thing is communicating the results to the community in a respected communication vehicle.
Our profession began talking about this at least 37 (thirty-seven) years ago, when we said, “Concern that sharing information with patients may cause sustained psychological distress is probably unfounded.”
In their comments and discussion, this research team anticipates that the wait will end, and I agree with them.
6 Comments
[…] Article Ted Eytan, MD, 25 July 2010 Article (Delbanco 2010) SHARETHIS.addEntry({ title: "Now Reading: “Patient review (of doctors’ notes) remains the rare exception, and roadblocks abound” : OpenNotes Project (Annals of Internal Medicine)", url: "http://articles.icmcc.org/2010/07/25/now-reading-%e2%80%9cpatient-review-of-doctors%e2%80%99-notes-remains-the-rare-exception-and-roadblocks-abound%e2%80%9d-opennotes-project-annals-of-internal-medicine/" }); […]
I have been thinking about progress notes a lot lately, and I think one of the main issues to address is their purpose. What if you were writing a mission statement for a progress note? What would that mission say?
Right now, most doctors don't think of their notes in that way. Many notes are a brief synopsis of the salient medical facts, with the appropriate amount of history, review of systems elements, physical exam, and assessment/plan to justify whatever billing code the doctor chose.
But what if notes were co-created between doctor and patient? What if they were shared notes? The patient could begin a note before even seeing the doctor. They could use the last note or the patient's care plan as a starting point, and together they could record what they believe is important. The assessment/plan could also be written together during the visit and the patient could leave with a copy of the completed note. The doctor is finished charting and the patient leaves with more and better information.
Shared notes. What would be their mission?
Now Reading: “Patient review (of doctors’ notes) remains the rare exception, and roadblocks abound” : OpenNotes Project http://is.gd/dLb6G
check out Ted Eytan's thoughtful post on #OpenNotes Project http://is.gd/dLb6G (via @bfm)
"When did you actually 'learn' that patients were not supposed to see their medical records?" – @Tedeytan on #OpenNotes http://bit.ly/9ZPtlj