I attended a smallish get together yesterday organized by Christine Kraft to think about Health 2.0 / DC in the epicenter type things, where we thought about some of the trends in social media use, social media use by physicians and medical groups (I got a lot of help on this one), journalists, and finally, a real story about a patient’s experience, here in DC, that really brings to light a problem with a meaningful use definition that doesn’t include “and the patients can see the data.”
I’ve been thinking about the idea that meaningful use must include “patients can see everything” since ARRA came out, and see my first mention of it in the Twittersphere around April 22. I have noticed since then that the idea seems to be picking up steam – initially I was told by some that this would be a “distraction” to the conversation. Now I’m sure that it’s not. Read on…
This is the story of Regina Holliday – it’s really worth a read, and I’ll quote some of it here:
We will fight the good fight. Regina’s USA medical advocacy 2009
Why do we have more transparency in special education law then in medical care? Why do we have more access to information on a box of Cheerios then on a medical chart? Why isn’t there a medical counterpart of the Freedom of Information Act? People tell me just concentrate on your husband, your family. Too many people have quietly done that. Too many wonderful fathers, mothers and children are gone. Too many graves have flowers on them. I will fight. I will not stop. I will not be silenced.
Regina told us her story in person, accompanied by the notebook of her husband’s medical record, which she was only allowed to get on paper, at $0.73 a page:

What struck us so much was the fact that his all started just a few weeks ago on March 27, 2009. A life threatening diagnosis creates an amazing call to action. As we learned about all the different ways that her husband’s care was potentially impacted by lack of information, our mood became more and more somber.
Regina happens to be an artist, and what she’s doing with her experience is as impressive as the challenge that she and her family is facing. At Washington, DC’s Pumpernickels Deli, she’ll be painting a mural of the Medical Facts of her husbands kidney cancer, patterned after the nutritional facts label.

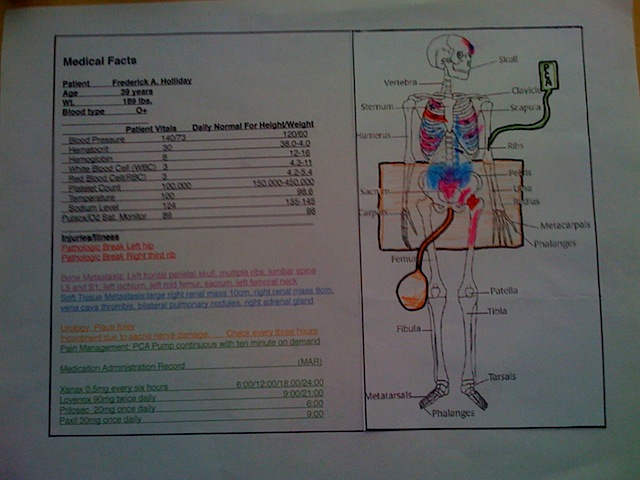
The installation will be large (6 feet tall), in color, and will be permanent. It may just become a monument to information disparity in health care. Regina told us that the mural may be completed by this week. It will be interesting to see the reaction of the community to the art piece.
In the meantime, I still think it’s worth asking:
- Is e-prescribing as meaningful as it should be, if patients and families can’t review what’s prescribed and know what they are supposed to be taking?
- Is interoperability meaningful if it only connects doctors to doctors, hospitals to hospitals, and not patients to their health information?
- Are quality metrics meaningful if patients do not get to see them and use them to make decisions about how their care is delivered?
Finally, if all of the things that are currently being cited as meaningful use not reviewable by the people whom they matter to most, the patient, what’s the incentive for anyone to make sure they are accurate? Everyone prizes accuracy, and the best organizations in the world know that the way to ensure it is to make sure that people who generate information see the impact of what they do.
It reminds me of this quote:
“The key to the success of Ryanair and other low-cost airlines, lies in the way they think about combining processes. Ryanair’s cabin crews also do the cleaning inside the aircraft, so if they make a bad job of it they have to face complaints from passengers. In more traditional airlines the cleaners never see the passengers.”
– Yves Morieux, Boston Consulting Group
Comments, as always, welcome. As well as a trip to the Pumpernickels Deli….
42 Comments
Great post, Ted!
And a fantastic title! This is the best definition yet of "meaningful use". There is always greatness in simplicity.
Regina's story is just one more example of why to produce useful reform of the healthcare system in 2009 you MUST put the patient at the center of it all.
Without it nothing will work because a large percentage of the American population has become equipped with the tools that will transform almost instantly anyone, from an apathetic member of the public into an engaged, empowered and therefore demanding e-patient.
Thank you, Ted, for recording Regina's story and how it fits into the larger context of the ARRA debate.
I continue to believe that health care reform is too big for most people to grasp, but through stories – and art! – people can begin to understand the implications of the debate. I'm still not over the way Regina talked about her request for information and was told to wait… and then pay 73 cents a page.
I want to say thank you, too, for this. I know so many who are treated like Regina and her husband. I am encouraging other patients to come read both sites.
Putting the patient in the middle of/in the center of/as the focus of healthcare reform? Why has it taken us this long?
Is it meaningful if patients can’t use it?: I attended a smallish get together yesterday organized by Christine .. http://tinyurl.com/mzg4z6
Is it meaningful if patients can’t use it? New post by @tedeytan about @ReginaHolliday and ARRA http://is.gd/IuWw
Terrific post, Ted, and pivotal question.
I'm disappointed but not surprised by the absence-of-consumers in the healthcare and IT posturing. A deafening silence…
We also need the other side of the story – where people get access to their information, and it makes a difference in their lives. Success at meaningful use by consumers may prove to get greater traction.
Reading: "Is it meaningful if patients can’t use it? | Ted Eytan, MD" ( http://tinyurl.com/ntjs7a )
This is among the most meaningful posts on “meaningful use,” from @tedeytan (who else?!) – The Story of Regina – http://bit.ly/OBC5F
“Why do we have more access to information on a box of Cheerios then on a medical chart?” The Story of Regina – http://bit.ly/OBC5F Wow.
“Why do we have more access to information on a box of Cheerios then on a medical chart?” The Story of Regina – http://bit.ly/OBC5F Wow.
Thank you, Ted, for so eloquently capturing Regina and Fred's story! Since meeting Regina on Wednesday I've been thinking about the letter vs. the spirit of the law. The hospitals gave the Hollidays access to Fred's chart: at 73 cents a page, and in an effectively unuseable format. Most EHRs I've seen, including my own, also comply with the letter, but not the spirit — the spirit of access and openness that would transform health information. I'm hopeful that Regina and Fred's story will help other see that what we need is more spirit.
@cindythroop The tiny.cc servers seem to be down. The tiny.cc/brushstroke post is aka http://is.gd/J4ij (on @TedEytan blog)
RT @cindythroop: For background on @ReginaHolliday and her recent/current experience with health care, read http://tiny.cc/brushstroke
Ted thank you for letting world read about my brother's fight and all Regina has done to keep him alive. My family has been through so much in these few months and they would also like to thank you. What Regina is doing is amazing and wish and pray for her to have all the power and strength to proceed and win.
The Brush Stroke Heard Around the World – background http://tiny.cc/brushstroke by @TedEytan (thx for asking @epatientdave!) #nwnw
For background on @ReginaHolliday and her recent/current experience with health care, read http://tiny.cc/brushstroke
Tiny.cc servers acting up…alternate link for "brush stroke" is http://is.gd/J4ij Thx @ePatientDave @ReginaHolliday
It’s official, @cindythroop broke the link to Ted Eytan’s post http://tiny.cc/brushstroke –> http://is.gd/J4ij (try second url)
Thank you for taking interest in the Holliday case. Regina is doing something positive in a very difficult situation. We will all benefit from the work she is doing. The more support we can all give in contacting our representatives in congress, the more we can support this cause.
RT @nancyshute: RT @cindythroop: Background on @ReginaHolliday and current experience with health care, read http://is.gd/J4ij (new URL)
Just wanted to make one clarification. I went to medical records and asked for the chart and was quoted .73 a page and a 21 day wait. This price would have been prohibitive especially as they told me I would need to pay even if there was duplication of parts of the record. Due to a paperwork snafu upon transfer I got to get a "free" copy of the record when the admitting hospital put it into my hands for safe keeping after I went back to the transferring hospital to have them print it out. If I had waited for the traditional record process I would have just gotten a copy of the record just as we were entering hospice…three hospitals later.
Thanks, Regina
Thanks Regina, Carrie, all, for your comments – they are very humbling to me, considering that it is you that are taking time from your lives (against your will) to help others.
I'm looking forward to my visit to the Pumpernickel and I hope others will learn from you too, the time is right,
Ted
[…] There is a growing discussion on the health consumer-centric (patient-centric) meaning of “meaningful use” of EHRs and health information technology. Jane Sarasohn-Kahn summarizes this discussion in her recent post, “Meaningful USe – or, whose health is it, anyway?” at Health Populi where she reflects on Ted Eytan’s post, “Is it Meaningful If Patients Can’t Use It?” […]
Meaningful use & patient safety: the power of consumers voices. Quick read of compelling example from @tedeytan http://bit.ly/lF143
RT @SafetyNurse Meaningful use & patient safety: the power of consumers voices. Quick read from @tedeytan http://bit.ly/lF143
Hi Ted,
In our brief experience learning about Kaiser and its online health manager, it seems that as an organization you folks at Kaiser are attacking each of the questions you're posing head on and making significant progress. Keep up the good work and influence change in DC!
You've been featured in a couple videos that The Doctor's Channel has recently posted. You can view them here:
Communicating with Patients Online
http://www.thedoctorschannel.com/video/1945.htm
Health 2.0 Meets Ix highlights
http://www.thedoctorschannel.com/video/1956.html
RT @SafetyNurse Meaningful use & patient safety: the power of consumers voices. Quick read from @tedeytan http://bit.ly/lF143 (expand)
Over many years I've come to learn a lot about medical records, mine for example. I have reqested a copy of my records and upon reading them I was shocked at the number of typographical errors in all of them. I did work as a Medical Transcriptionist and was very proud of the work I did. Due to the fact that my Mother had cancer and passed in 1975 we were able to get her medical records while she was alive, at no cost. I have since read these records and was astonished at the number of errors made in her medical care. My Dad passed away 2 years ago, during the prior 10 years I asked for his medical records and received them also at no cost. My Dad was 90, yet after reading these records and understanding what I was reading learned of the many errors regarding his care by primary care doctor, specialists, hospitals, nursing home and more.
On top of all of this I am 100% disabled, have been since 1970. I too, have most of my medical records, old RX bottles, x-rays, mri's, other tests, actual MRI's themselves with typed reports. H&P's, OR reports, hospital stay reports with nurses notes, discharge diagnoses, and much more. When a patient says they cannot afford a test, the physicial dictates that the patient refuses the test. Medicare is 80/20, most of the time on SSD did not have the 20% to have these tests. Companies that performed these tests denied me because of the 20%, now where is anything that states I refused anything because I just didn't want it. Money speaks louder than I do.
I had an HMO on several occasions, denied MRI's because the HMO company said I did not need it. Now my spine is so deteriorated no one can do anything for me. Someone behind a desk not knowing anything about medicine decided that NO MRI should be done. Yet a orthopaedic physician/surgeon who went to school for many years said I needed this test, yet I could not. Who was the one that ended up suffering because of an uneducated person in the field of Orthopaedics said NO, I suffered, am still suffering and always will. Have pain, severe, chronic, 24/7 for so many years, 1970 thru today, 6.14.09 taking heavy duty pain medication that I so wish I could throw away, but I can't. I need to get out of bed and walk, i have a mind, I am fairly intelligent. Have taught myself how to use a computer. I remember my medical terminology, if i don't know what something is, i look it up.
There are many senior citizens who have medical records that are incomplete and/or incorrect. I had learned of many ways of getting our medical records without paying for them, took many years, but I can still do it. I have received diagnoses for friends from their doctor's offices without the patient's permission. This is against the law, but the people did not believe me. When working we had to call the patient back, after their inquiry, ask them a question that was on their chart to verify it was the patient who was calling.
There is so much more. Just one last thing, my records from Medicare after the HIPPA act was put into place, and I signed it that no one could get anything about my medical care without my permission, I had found out that an attorney received my medical records from Medicare because they made an error and sent them. Medicare agreed that they made an error in sending this information out. Without money I could not hire an attorney to sue Medicare, even Medicare said I should sue them for viollation of my human rights. What a joke this all is.
I would very much like to do more about this, to help others, but I have no idea how. I have friends calling me to ask me medical questions, and i reply to the best of my ability, but also tell them to ask their physician, get as much information as they can ont he pc, at the library, a 2nd opinion from another doctor. Check their medical records charts to see if any errors had been made in typing, if so have them changed, which is now legal. A patient has every right to ask to look at their own chart while in the hospital and at the physician's office. It is their right, and totally legal for them to look at it. If told no, then whoever it is that said no, is wrong, and something can be done. Most people have no idea about any of this. They need to be taught. Those who don't go to doctors much, need to taught this information. I am unable to work but I know there is something I can do in this area. I am a baby boomer, age 61, born in 1947. Will never be without pain because 2 physicians that performed surgery made errors, and because it took 7 years to diagnose what was wrong the statute of limitations in this state was over. 4 years even from date of discovery. How sad i cannot lead a half-way normal existance because someone was practicing a spinal procedure on me, which i was lied to about it, and it did not work, infact its worse and get moreso every year i live.
I am a physician, and everytime a patient asks for something, I never ever hesitate to print it out (using own paper, printer, toner, etc). I don't understand what all the fuss is about.
Have any of you asked for records and not received them?
I think the question is about the barrier to asking. In a typical week, what % of your patients leave the office with a copy of the records generated from their visit?
[…] element), while we, sitting in a country that prides itself to be the most advanced in the world, cannot, in general, have access to any of our health data without delay and at no […]
I just left a hospital tonight and requested to just view my sister's chart to get a more accurate picture of what was going on with her, since she has 3 different doctors. She also had no clue as to what was going on with health or any type of diagnosis. My sister gave the nurse the authority to let me see her chart. I was told that I could not see it unless I had an order from her Dr. allowing me to see it. I told them that I did not want to take the chart anywhere, I wanted to just stand at the nurse's station and review her admission orders to get an idea of what was going on with her. By the way, I have a medical and legal background. I was not allowed to see her chart. So, I totally agree that there needs to be something done to get more access for the patient and patient's family.
Dori, Trena/all,
Thank you for these stories, and I hope more are posted – feel free to use this blog space to add them. I think it is unfortunate that there's a misunderstanding sometimes that patients and their families are committed to the wellbeing of their loved ones and the health care system at the same time. When we think that way, it's less important that someone be "right" than that the care is "accurate."
This article and story just published in the Harvard Business Review is very relevant here, in my opinion. When pilots/leaders learn to be inclusive, they are more likely to make the right decisions for those who they are caring for. And what physician, nurse, patient or family doesn't want that,
Ted
http://twitpic.com/dsrt2 – Howard Dean reading @tedeytan’s blog post http://tinyurl.com/ntjs7a
These stories have touched me in so many different ways. Regina's account of the events leading up to her husband's death are tragic and truly heartbreaking. I sit and cry for a family that I have never met and the knowledge that those they depended on during this trying time, let them down in unimaginable ways. How do you deal with watching a loved one suffer while at the same time deal with the inadequacies of our health care system and those that are a part of it? When and where will this end? When those "in charge" and those who "matter" are forced to bear similar circumstances as those of Regina and Fred? When their loved ones share a similar, unfortunate fate? Will this issue suddenly become more "important" or will those families be spared based solely on a well-known last name or the financial means to warrant more human treatment?
Dori's story was especially significant to me because I am the owner of a medical transcription company, with 28 girls around the country working for me very long hours, practicing my craft for 30+ years, and working 7 days a week, sometimes 14-18 hours a day, just to ensure that the files of every, single patient are accurate so that physicians and/or patients can rely on this information so that the best possible continued medical care will be provided based on their medical records to date. When all transcription work is brought back to this country, as it should always have been, in my opinion, there will be significant positive changes seen with regard to this specific issue. This will be just one small, but important, step in avoiding stories like Dori's and I'm sure what amounts to thousands of others…and when you add small steps together then they enable us to reach what we thought were insurmountable heights in many instances, and I am sure that this would also be true for health care…the system is so broken and needs to be fixed before it does reach that insurmountable distance – before stories like Regina's and Fred's overtake us as a society. None of us are immune to becoming one of these statistics – and none of us should ever have to bear the sorrow of being on a borrowed ladder, with donated paint and used paintbrushes…just to make such a valid point and get the rest of us to listen.
[…] blatantly stole that line from Ted Eytan whose post, Is it meaningful if patients can’t use it?, chronicles our first meeting with Regina Holliday (who was featured in an NPR story by Joseph […]
[…] health care reform debate. Compare these photos of a medical record from 1934 to those that cost .73 cents today. Could today’s physician and his or her patient get “meaningful use” out of this […]
As a cancer survivor, this type of thing is the reason we need immediate attention to our healthcare system. I don't know what the right answer is, but what we have isn't it!!
[…] I first posted about this issue in May, 2009, when I met Regina Holliday. , and as I have also mentioned previously, meaningful use as defined in the ARRA law did not include patient and family engagement – the HIT Policy Committee added it, which says great things about our accumulated experience with health information technology to date. […]
Thank You. @paintmd (What did @tedeytan say in May '09?) "Is it meaningful if patients can't use it? https://www.tedeytan.com/2009/05/28/3086
RT @ReginaHolliday: Thank You. @paintmd (What did @tedeytan say in May '09?) "Is it meaningful if patients can't use it? https://www.tedeytan.com/2009/05/28/3086
[…] There is a growing discussion on the health consumer-centric (patient-centric) meaning of “meaningful use” of EHRs and health information technology. Jane Sarasohn-Kahn summarizes this discussion in her recent post, “Meaningful USe – or, whose health is it, anyway?” at Health Populi where she reflects on Ted Eytan’s post, “Is it Meaningful If Patients Can’t Use It?” […]